

A 29 y/o HIV positive male presents with dyspnea, dry cough and right sided chest pain since yesterday. The chest pain is worse when he takes a deep breath or coughs. He has chills and night sweats for the past week, which was attributed to the flu. He has been hospitalised several times in the past for heroin overdose. 5 months ago, he was admitted and treated for aspiration pneumonia. Last year, he was also admitted for cocaine overdose complicated by tonic-clonic seizures. His most recent CD4 count is 190/mm³. He has no drug allergies.
In the ED, he appears slightly uncomfortable and has shallow breathing.
BP 105/70 mmHg
HR 110 bpm and regular
RR 22 bpm
SpO2 95% on room air
Temp 39.4° C
BMI 19 kg/m²
There are multiple needle tracks and a tender subcutaneous mass in the right antecubital area. The neck veins are flat when the patient is in a semi-recumbent position. A 2/6 systolic murmur is heard at the left sternal border. Liver is palpated 1cm below the costal margin and is non tender. A chest X ray shows nodular opacities in both lung fields, including sub pleural opacities on the right.
Serum K 3.8
Creatinine 1.0
Blood cultures are obtained and IV fluids are started.
Which of the following is most likely to establish the diagnosis in this patient?
0%Bronchoscopy with BAL
0%CT angiography of the chest
0%Sputum Induction
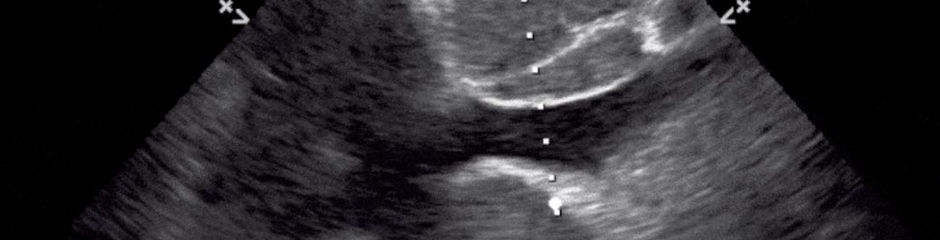
0%Transthoracic Echo
The answer over here is a transthoracic echocardiogram.
Patient most likely has acute right sided IE. Although left sided IE is more common in the general population, those who use IV drugs most commonly develop right sided IE affecting the tricuspid valve.
Staph aureus is the most common cause >50% of the cases. Presentation is typically acute and characterized by high fevers. They often have pleuritic chest pain and cough d/t septic pulmonary emboli, a complication that occurs in 75% cases of right sided IE. The emboli appear on CXR as multiple nodular opacities. Cardiac murmur is sometimes absent in right sided IE and peripheral signs of IE are also not present.
So initially a TTE is done, followed by TEE if indicated.
Patient is at risk for Pneumocystis pneumonia and a bronchoscopy with BAL is used for diagnosis. However, that presentation is usually subacute (3 weeks, low grade fever, non productive cough) and CXR usually shows interstitial infiltrates rather than nodular opacities.