

CRITICAL CARE TRIALS
Stay ahead of the curve with exciting new clinical trials from the critical care field presented in vivid, visual abstract format. Gain comprehensive and insightful perspectives as each critical development is delivered to you.

Jun 23, 2022
LOVIT Trial
Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit.
In a multicenter RCT of 872 septic ICU patients on vasopressors, intravenous vitamin C increased the risk of death or persistent organ dysfunction at 28 days compared to placebo (44.5% vs. 38.5%; RR 1.21, 95% CI 1.04–1.40, P = 0.01). Mortality (35.4% vs. 31.6%) and organ dysfunction rates were higher but not statistically significant. No safety concerns were noted. These findings do not support the use of intravenous vitamin C in sepsis management.
127

Jun 17, 2022
CLASSIC Trial
Restriction of Intravenous Fluid in ICU Patients with Septic Shock.
In a multicenter RCT of 1554 patients with septic shock, a restrictive fluid strategy did not reduce 90-day mortality compared to standard fluid therapy (42.3% vs. 42.1%; adjusted difference 0.1 percentage points, 95% CI -4.7 to 4.9; P = 0.96). Serious adverse events and secondary outcomes were similar. These findings support continued use of standard fluid strategies per the Surviving Sepsis Campaign guidelines until further evidence warrants guideline modification.
250

Jun 16, 2022
PREPARE II Trial
Effect of Fluid Bolus Administration on Cardiovascular Collapse Among Critically Ill Patients Undergoing Tracheal Intubation.
In a multicenter RCT of 1065 ICU patients undergoing endotracheal intubation, a 500-mL fluid bolus did not significantly reduce vascular collapse compared to no fluid bolus (21.0% vs. 18.2%; absolute difference 2.8%, 95% CI -2.2% to 7.7%; P = 0.25). Secondary outcomes, including 28-day mortality (40.5% vs. 42.3%), were also similar. These findings suggest routine fluid bolus administration does not prevent vascular collapse during intubation.
41

Jun 15, 2022
TTM & TTM2 Meta-analysis
Hypothermic versus Normothermic Temperature Control after Cardiac Arrest.
In a meta-analysis of 2800 patients from the TTM and TTM2 trials, hypothermia at 33°C did not reduce 6-month all-cause mortality compared to normothermia (49.4% vs. 47.9%; RR 1.03, 95% CI 0.96–1.11, P = 0.41) or improve neurological outcomes (54.3% vs. 54.0%; RR 1.01, 95% CI 0.94–1.08, P = 0.88). No subgroup showed benefit with hypothermia. Evidence supports device-controlled normothermia (36–37.8°C) after out-of-hospital cardiac arrest.
71

May 18, 2022
TTCOV19
Timing of tracheotomy in SARS-CoV-2-infected patients: a multicentre, single-blinded, randomized, controlled trial.
In a multicenter RCT of 150 COVID-19 patients requiring mechanical ventilation, early tracheostomy (≤7 days) did not significantly reduce total ventilator days compared to late tracheostomy (≥10 days) in the ITT analysis (19.6 vs. 21.1 days; P = 0.5). PP analysis showed fewer ventilator days with early tracheostomy (22.3 vs. 30.3 days; P = 0.0064). Mortality and ICU length of stay were similar. While underpowered, early tracheostomy may be considered for select patients needing prolonged ventilation.
23
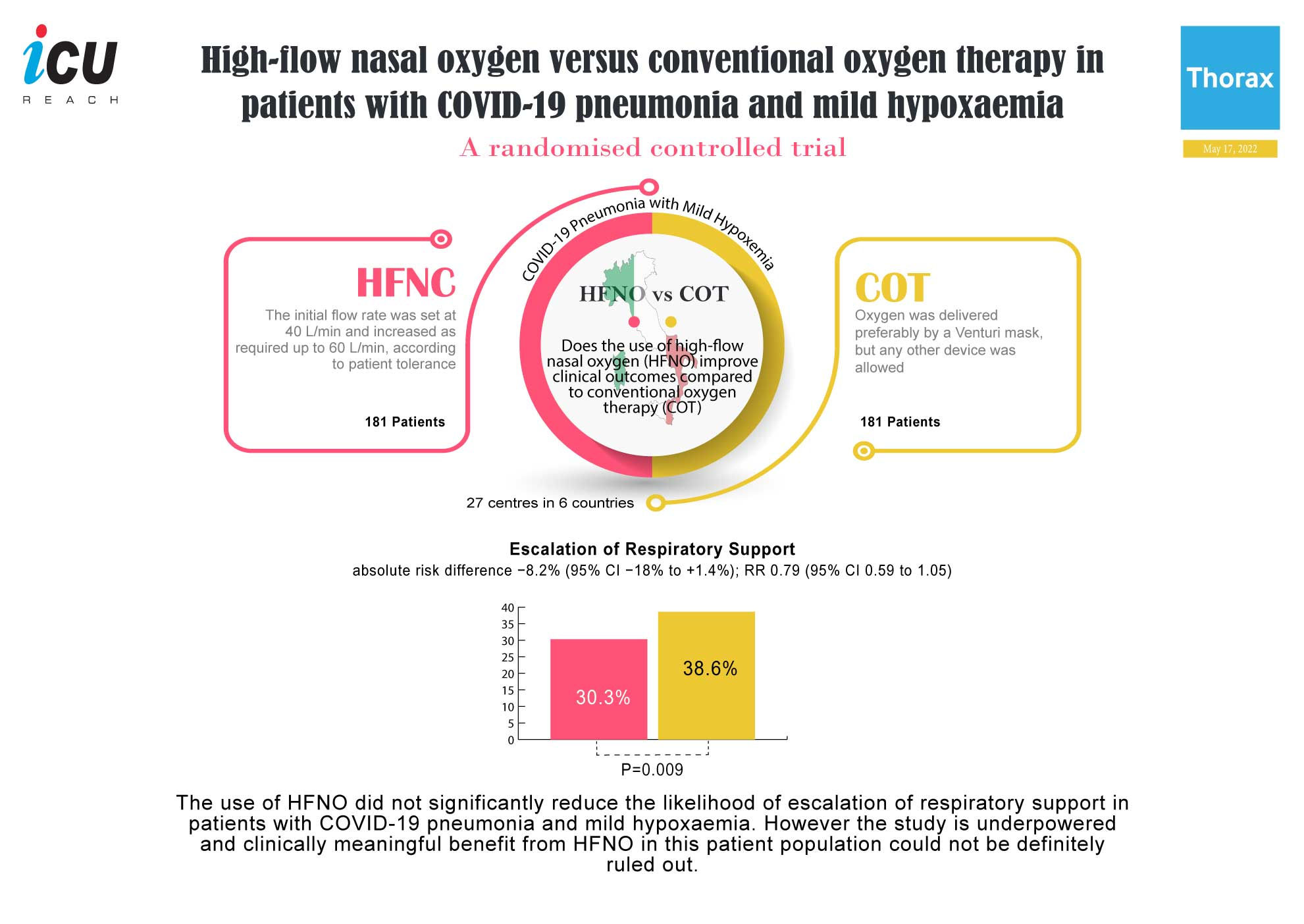
May 17, 2022
HFNO vs COT in COVID-19 Pneumonia
High-flow nasal oxygen versus conventional oxygen therapy in patients with COVID-19 pneumonia and mild hypoxaemia: a randomised controlled trial.
In a multicenter RCT of 362 patients with COVID-19 pneumonia and mild hypoxemia, high-flow nasal oxygen (HFNO) did not significantly reduce the escalation of respiratory support compared to conventional oxygen therapy (30.3% vs. 38.6%; P = 0.09). Secondary outcomes, including clinical recovery and ICU admission, were similar. The study was underpowered, so a potential clinically meaningful benefit of HFNO cannot be definitively excluded.
50

May 15, 2022
COVI-PRONE Trial
Effect of Awake Prone Positioning on Endotracheal Intubation in Patients With COVID-19 and Acute Respiratory Failure.
In a multicenter RCT of 400 patients with COVID-19 and hypoxemic respiratory failure, awake prone positioning did not significantly reduce 30-day intubation rates compared to usual care (34.1% vs. 40.5%; P = 0.20). Secondary outcomes, including 60-day mortality and ventilator-free days, were also similar. While the study did not achieve its target prone duration, a clinically meaningful benefit cannot be excluded. Awake prone positioning remains a reasonable intervention for pre-intubation hypoxemic respiratory failure.
56

May 4, 2022
SETPOINT2 Trial
Effect of Early vs Standard Approach to Tracheostomy on Functional Outcome at 6 Months Among Patients With Severe Stroke Receiving Mechanical Ventilation.
In a multicenter RCT of 382 mechanically ventilated patients with severe stroke, early tracheostomy (≤5 days) did not significantly improve 6-month functional outcomes without severe disability (mRS ≤4) compared to standard tracheostomy (43.5% vs. 47.1%; OR 0.93, 95% CI 0.60–1.42; P = 0.73). Serious adverse events were similar between groups. Findings suggest no clear benefit of early tracheostomy, though a smaller effect cannot be excluded due to wide confidence intervals.
113

Apr 7, 2022
FIRST-ABC Trial
Effect of High-Flow Nasal Cannula Therapy vs Continuous Positive Airway Pressure Following Extubation on Liberation from Respiratory Support in Critically Ill Children.
In a multicenter trial of 553 critically ill children requiring non-invasive respiratory support post-extubation, HFNC (50.5 hrs) failed to demonstrate non-inferiority to CPAP (42.9 hrs) for time to liberation from respiratory support (adjusted HR 0.83; 1-sided 97.5% CI, 0.70–∞). Secondary 180-day mortality was higher with HFNC (5.6% vs. 2.4%). Findings suggest CPAP may be preferred for post-extubation respiratory support in young childre
83

Apr 5, 2022
Esmolol in Septic Shock Patients
Esmolol to Treat the Hemodynamic Effects of Septic Shock: A Randomized Controlled Trial.
In a phase II trial of esmolol for septic shock, no significant differences were found in norepinephrine-equivalent dose, time to shock reversal, or inflammatory markers (except lower CRP in the esmolol group). Reduced oxygen consumption was noted in a subset of esmolol patients. While prior studies suggested improved hemodynamics and mortality benefits, this trial highlights the need for a large, well-powered RCT to evaluate patient-centered outcomes of esmolol in septic shock.
147

Mar 7, 2022
RePHILL Trial
Resuscitation with blood products in patients with trauma-related hemorrhagic shock receiving prehospital care.
In a multicenter RCT of 432 patients with hemorrhagic shock and hypotension, pre-hospital resuscitation with blood products (PRBC and lyophilized plasma) did not significantly improve composite outcomes of mortality or impaired lactate clearance compared to normal saline. Individual components of the composite outcome also showed no difference. Findings suggest no advantage of blood products over saline for pre-hospital resuscitation in this setting.
53

Mar 3, 2022
PLUS Trial
Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults.
In a multicenter RCT of 5037 critically ill patients, balanced multielectrolyte solution (BMES) did not significantly reduce mortality (21.8% vs. 22.0%) or the need for renal replacement therapy (12.7% vs. 12.9%) compared to saline. Serum creatinine changes were similar between groups. Findings suggest no clinical advantage of BMES over saline for critically ill patients, though limitations warrant consideration in specific contexts.
70