

CRITICAL CARE TRIALS
Stay ahead of the curve with exciting new clinical trials from the critical care field presented in vivid, visual abstract format. Gain comprehensive and insightful perspectives as each critical development is delivered to you.
Feb 24, 2022
TELSTAR Trial
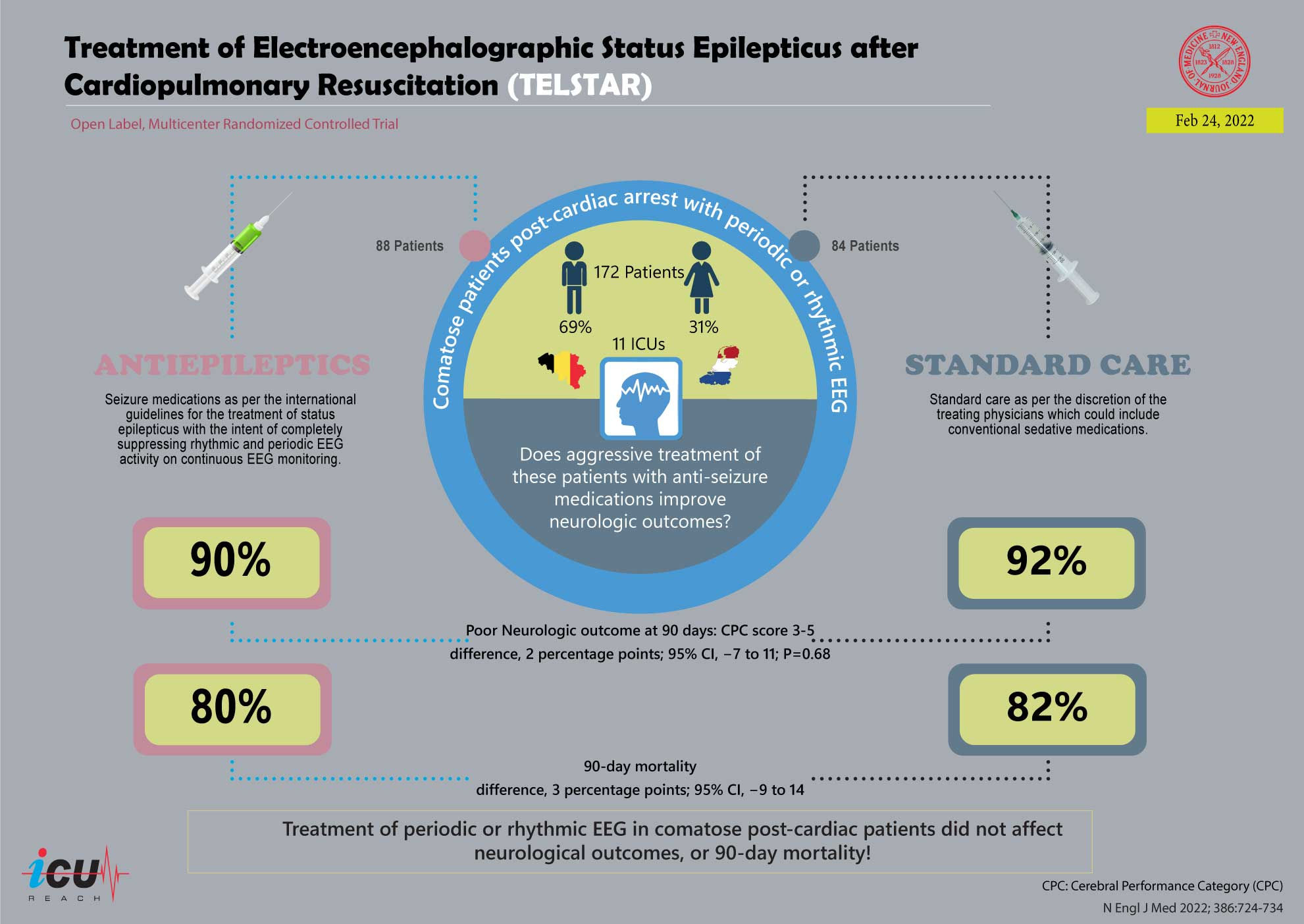
Treating Rhythmic and Periodic EEG Patterns in Comatose Survivors of Cardiac Arrest.
In a multicenter RCT of 172 comatose cardiac arrest survivors, intensive anti-seizure treatment to suppress rhythmic/periodic EEG activity did not improve poor neurologic outcomes at 3 months (90% vs. 92%; P = not significant) compared to standard care. Mortality was similarly high (80% vs. 82%). The anti-seizure group had longer ICU stays and ventilation duration, with >80% of patients experiencing serious adverse events in both groups. Findings do not support aggressive EEG suppression in this population.
77

Feb 10, 2022
CHOICE Trial
Effect of Intra-arterial Alteplase vs Placebo Following Successful Thrombectomy on Functional Outcomes in Patients with Large Vessel Occlusion Acute Ischemic Stroke.
In a phase IIb RCT of 121 patients with large vessel occlusion acute ischemic stroke who achieved successful reperfusion after thrombectomy, adjunct intra-arterial alteplase improved the likelihood of excellent neurological outcomes (mRS 0-1 at 90 days: 59.0% vs. 40.4%; P = statistically significant). These findings are promising but require validation in larger trials before altering clinical practice.
30

Jan 24, 2022
RECOVERY-RS Trial
Effect of Noninvasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19.
In a multicenter RCT of 1273 hospitalized patients with COVID-19-related acute hypoxemic respiratory failure, CPAP reduced the composite outcome of tracheal intubation or 30-day mortality compared to conventional oxygen therapy (36.3% vs. 44.4%; absolute difference −8%, 95% CI −15% to −1%; P = 0.03). HFNO showed no significant difference compared to COT (44.3% vs. 45.1%). Adverse events were higher with CPAP. CPAP may improve outcomes, while HFNO needs further investigation due to underpowering.
58

Dec 8, 2021
Bougie Trial
Effect of Use of a Bougie vs Endotracheal Tube With Stylet on Successful Intubation on the First Attempt Among Critically Ill Patients Undergoing Tracheal Intubation.
In a multicenter RCT of 1102 critically ill patients, the use of a bougie for intubation did not improve first-attempt success rates compared to a stylet (80.4% vs. 83.0%). Rates of severe hypoxemia (11.0% vs. 8.8%) and complications, including esophageal intubation (0.7% vs. 0.9%) and pneumothorax (2.5% vs. 2.7%), were similar. Findings suggest no advantage of bougie over stylet for first-attempt intubation under these conditions. Current practice remains unchanged.
55

Nov 30, 2021
COCA Trial
Effect of Intravenous or Intraosseous Calcium vs Saline on Return of Spontaneous Circulation in Adults With Out-of-Hospital Cardiac Arrest.
In a randomized trial of 397 adult patients with out-of-hospital cardiac arrest, intravenous or intraosseous calcium administration did not improve sustained return of spontaneous circulation (19% vs. 27%; P = 0.09) compared to saline. Survival at 30 days (5.2% vs. 9.1%; P = 0.17) and favorable neurological outcomes (3.6% vs. 7.6%; P = 0.12) were also lower in the calcium group. The trial was stopped early due to potential harm. Calcium should not be administered in this setting.
27

Sep 29, 2021
VAM-IHCA Trial
Effect of Vasopressin and Methylprednisolone vs Placebo on Return of Spontaneous Circulation in Patients with In-Hospital Cardiac Arrest.
In a multicenter RCT of 512 patients with in-hospital cardiac arrest, vasopressin plus methylprednisolone significantly improved return of spontaneous circulation (42% vs. 33%; RR 1.30, 95% CI 1.03–1.63; P = 0.03) compared to placebo. However, there was no difference in 30-day survival (9.7% vs. 12%; P = 0.48) or favorable neurologic outcomes (7.6% vs. 7.6%; P > 0.99). The study demonstrates short-term benefit but lacks evidence for long-term outcomes, and findings are unlikely to alter ACLS recommendations.
31

Aug 31, 2021
REST Trial
Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients With Acute Hypoxemic Respiratory Failure.
This multicenter RCT assessed whether lower tidal volume ventilation (≤3 mL/kg) with extracorporeal CO₂ removal (ECCO₂R) improves 90-day mortality in acute hypoxemic respiratory failure compared to conventional ventilation (6 mL/kg). Among 412 patients, in-hospital mortality was similar (41.5% vs. 39.5%, p=0.68), but ventilator-free days were fewer (7.1 vs. 9, p=0.02). Serious adverse events, including intracranial hemorrhage, were more common with ECCO₂R. The trial, underpowered due to early termination, does not support ECCO₂R use and highlights potential harm.
87

Aug 10, 2021
BaSICS Trial
Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients
The BaSICS trial was a multicenter, randomized controlled study involving 10,520 critically ill adults in 75 ICUs across Brazil. It compared the effect of balanced crystalloids (pH 7.4 isotonic solution) versus 0.9% saline for intravenous fluid resuscitation on 90-day mortality. Patients had at least one risk factor for worse outcomes and were expected to stay in the ICU for more than 24 hours. Death within 90 days occurred in 26.4% of the balanced solution group and 27.2% of the saline group. The difference was not statistically significant (adjusted HR 0.97; 95% CI, 0.90–1.05). The trial concluded that balanced solutions did not significantly improve 90-day survival compared with saline in this population.
9

Aug 10, 2021
BaSICS Trial
Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients.
In a multicenter RCT of 11,052 critically ill patients, the use of balanced solution (Plasma-Lyte 148) did not significantly reduce 90-day mortality compared to saline (26.4% vs. 27.2%; HR 0.97, 95% CI 0.90–1.05; P = 0.47). AKI requiring RRT and other secondary outcomes were similar. Subgroup analysis showed higher mortality with balanced fluids in traumatic brain injury patients. Findings suggest saline is safe for ICU patients, with balanced fluids avoided in traumatic brain injury.
116

Jun 17, 2021
TTM2 Trial
Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest.
In a multicenter RCT of 1861 comatose survivors of out-of-hospital cardiac arrest, targeted hypothermia at 33°C did not significantly reduce 6-month all-cause mortality compared to targeted normothermia with fever control (50% vs. 48%; P = 0.37). Functional outcomes were also similar (poor mRS: 55% vs. 55%). Hypothermia increased arrhythmias (24% vs. 17%; P < 0.001). These findings emphasize the importance of active temperature management and hyperthermia avoidance rather than hypothermia itself.
47

Apr 15, 2021
MENDS2 Trial
Dexmedetomidine or Propofol for Sedation in Mechanically Ventilated Adults with Sepsis.
In a multicenter RCT of 432 mechanically ventilated septic patients, dexmedetomidine did not improve days alive without delirium or coma compared to propofol (median 10.7 vs. 10.8 days). Ventilator-free days (23.7 vs. 24.0), 90-day mortality (38% vs. 39%), and 6-month cognitive outcomes (TICS-T scores: 40.9 vs. 41.4) were similar. Safety profiles were comparable. Findings support continued use of either sedative based on clinical preference or patient-specific factors.
105

Apr 8, 2021
HOT-ICU Trial
Lower or Higher Oxygenation Targets for Acute Hypoxemic Respiratory Failure.
In a multicenter RCT of 2928 ICU patients with acute hypoxemic respiratory failure, targeting a lower PaO₂ (60 mm Hg) did not reduce 90-day mortality compared to a higher target (90 mm Hg) (42.9% vs. 42.4%; P = 0.64). Secondary outcomes, including days alive without life support and ischemic events, were also similar. Findings support maintaining PaO₂ targets within the range of 60–90 mm Hg without favoring a lower target for improved outcomes.
90