

CRITICAL CARE TRIALS
Stay ahead of the curve with exciting new clinical trials from the critical care field presented in vivid, visual abstract format. Gain comprehensive and insightful perspectives as each critical development is delivered to you.

Oct 16, 2014
ARISE Trial
Goal-Directed Resuscitation for Patients with Early Septic Shock.
In a multicenter RCT of 1600 patients with septic shock, early goal-directed therapy (EGDT) did not significantly improve 90-day mortality compared to usual care (18.6% vs. 18.8%; P = 0.90). EGDT involved more fluids, vasopressors, transfusions, and dobutamine use. Usual care has evolved to include early antibiotics and adequate fluid resuscitation, making it as effective as EGDT. These findings support a less invasive approach for septic shock management
65

Oct 9, 2014
TRISS Trial
Lower versus Higher Hemoglobin Threshold for Transfusion in Septic Shock.
In a multicenter RCT of 1005 patients with septic shock, a low hemoglobin transfusion threshold (7 g/dL) did not significantly differ from a high threshold (9 g/dL) in 90-day mortality (43.0% vs. 45.0%; P = 0.44). The low-threshold group required fewer transfusions (median 1 vs. 4 units; P < 0.001). No differences were observed in ischemic events, adverse reactions, or ICU length of stay. Findings support a restrictive transfusion strategy (threshold 7 g/dL) in septic shock patients without active bleeding or acute coronary syndrome.
143
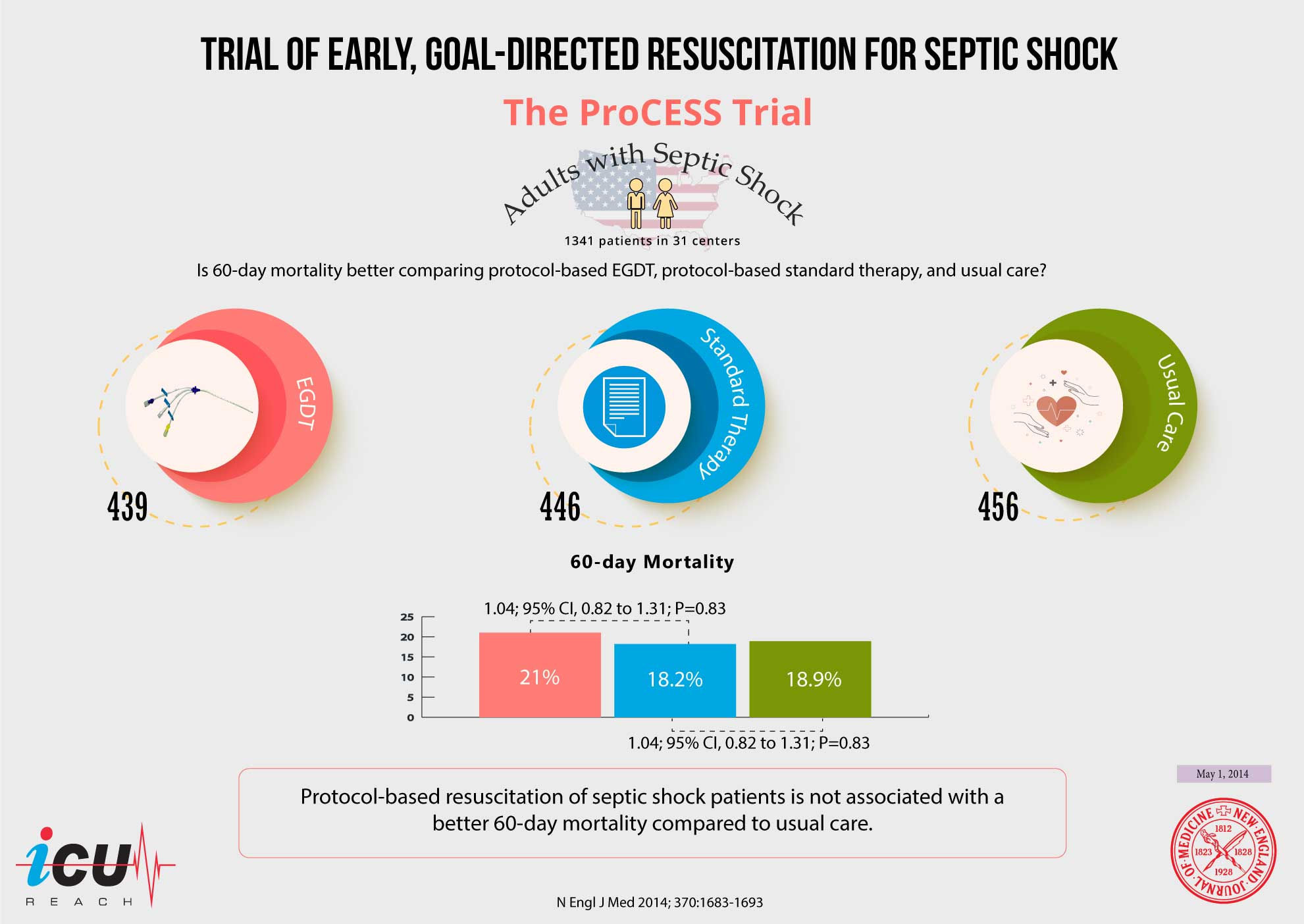
May 1, 2014
ProCESS Trial
A Randomized Trial of Protocol-Based Care for Early Septic Shock.
In a multicenter RCT of 1341 patients with septic shock, protocol-based EGDT, protocol-based standard therapy, and usual care showed no significant difference in 60-day mortality (21.0%, 18.2%, and 18.9%, respectively; P = 0.83). No differences were observed in longer-term mortality or organ support needs. These findings reflect advances in usual care, emphasizing early antibiotics and fluid resuscitation, and suggest that less invasive approaches are equally effective for septic shock management.
63

Apr 24, 2014
SEPSISPAM Trial
High versus Low Blood-Pressure Target in Patients with Septic Shock.
In a multicenter RCT of 776 patients with septic shock, targeting a higher mean arterial pressure (MAP) of 80–85 mm Hg did not reduce 28-day mortality compared to a lower MAP of 65–70 mm Hg (36.6% vs. 34%; P = 0.57). Secondary outcomes, including 90-day mortality, were also similar. In patients with chronic hypertension, high MAP reduced the need for renal replacement therapy (31.7% vs. 42.2%; P = 0.046). These findings support a MAP target of 65–70 mm Hg, with higher targets considered for hypertensive patients.
131

Apr 10, 2014
ALBIOS Trial
Albumin Replacement in Patients with Severe Sepsis or Septic Shock.
In a multicenter trial of 1818 patients with severe sepsis, albumin replacement targeting serum albumin ≥30 g/L did not reduce 28-day mortality compared to crystalloids alone (31.8% vs. 32%; P = 0.94) or 90-day mortality (41.1% vs. 43.6%; P = 0.29). Secondary outcomes were similar. Post hoc analysis suggested reduced 90-day mortality in septic shock patients with albumin (43.6% vs. 49.9%; P = 0.03). These findings do not support routine albumin replacement in severe sepsis, but further study in septic shock is warranted.
488

Apr 10, 2014
PEITHO Trial
Fibrinolysis for Patients with Intermediate-Risk Pulmonary Embolism.
In a multicenter RCT of 1005 normotensive patients with intermediate-risk PE, tenecteplase with heparin significantly reduced the composite outcome of death or hemodynamic decompensation within 7 days compared to heparin alone (2.6% vs. 5.6%; P = 0.02; NNT = 34), driven by reduced hemodynamic decompensation. However, major bleeding (6.3% vs. 1.2%; P < 0.001; NNH = 19) and hemorrhagic stroke (2% vs. 0.2%; P = 0.003; NNH = 55) were higher. Routine thrombolysis is not supported in submassive PE due to bleeding risks.
294

Dec 5, 2013
TTM Trial
Targeted Temperature Management at 33°C versus 36°C after Cardiac Arrest.
In a multicenter RCT of 939 patients with out-of-hospital cardiac arrest, targeted temperature management at 33°C did not significantly differ from 36°C in mortality at the end of the trial (50% vs. 48%; P = 0.51) or in poor neurologic outcomes at 180 days (54% vs. 52%; P = 0.78). These findings support active temperature management and avoidance of hyperthermia as key factors for improved outcomes in cardiac arrest survivors, regardless of the specific temperature target within this range.
52

Jun 6, 2013
PROSEVA Trial
Prone Positioning in Severe Acute Respiratory Distress Syndrome.
This multicenter RCT investigated prone positioning (≥16 hours/day) versus supine positioning in 466 patients with moderate to severe ARDS (PaO₂/FiO₂ <150, FiO₂ ≥0.6, PEEP ≥5). Prone positioning significantly reduced 28-day mortality (16% vs. 32.8%, HR 0.39, 95% CI 0.25–0.63, p<0.001) and improved 90-day outcomes, extubation rates, and ventilator-free days, with no increase in adverse events. Despite baseline imbalances, the study established prone positioning as a standard of care in ARDS.
224

Feb 28, 2013
OSCAR Trial
High-Frequency Oscillation for Acute Respiratory Distress Syndrome.
This multicenter RCT evaluated high-frequency oscillation ventilation (HFOV) versus conventional mechanical ventilation in 795 ARDS patients (PaO₂/FiO₂ <200). 30-day mortality was similar between groups (41.7% vs. 41.1%, p=0.85), with no difference in ventilator-free days, ICU/hospital length of stay, or vasopressor use. HFOV improved oxygenation (PaO₂/FiO₂: 212 vs. 163 on Day 2) but required longer neuromuscular blockade (2.5 vs. 2 days, p=0.02). Limitations include lack of mandatory ARDSNet protocol and inexperience with HFOV. Routine HFOV use in ARDS is not supported.
173

Feb 28, 2013
OSCILLATE Trial
High-Frequency Oscillation in Early Acute Respiratory Distress Syndrome.
This multicenter RCT compared high-frequency oscillation ventilation (HFOV) with conventional low tidal volume ventilation in 548 patients with moderate to severe ARDS (PaO₂/FiO₂ <200). In-hospital mortality was higher in the HFOV group (47% vs. 35%, RR 1.33, 95% CI 1.09–1.64, p=0.005). HFOV patients required more sedatives, neuromuscular blockers, and vasoactive drugs. Despite less refractory hypoxemia, HFOV was associated with harm, leading to its decline in practice. ECMO is favored for refractory hypoxemia.
65

Nov 15, 2012
CHEST Trial
Hydroxyethyl Starch or Saline for Fluid Resuscitation in Intensive Care.
In a multicenter RCT of 7000 critically ill patients, resuscitation with 6% HES (130/0.4) did not significantly reduce 90-day mortality compared to saline (18% vs. 17%; P = 0.26). HES increased the need for renal replacement therapy (7.0% vs. 5.8%; P = 0.04, NNH = 83) and acute kidney injury (38.0% vs. 34.6%; P = 0.005) and was associated with more adverse events, including pruritus and rash. These findings suggest HES should not be used for fluid resuscitation in critically ill patients.
113

Jul 12, 2012
6S Trial
Hydroxyethyl Starch 130/0.42 versus Ringer's Acetate in Severe Sepsis.
In a multicenter RCT of 804 patients with severe sepsis, fluid resuscitation with 6% HES (130/0.42) significantly increased the composite outcome of 90-day mortality or dependence on dialysis compared to Ringer's acetate (51% vs. 43%; P = 0.03, NNH = 13). HES also increased the need for renal replacement therapy (22% vs. 16%; P = 0.04, NNH = 17). These findings strongly discourage the use of HES for resuscitation in septic ICU patients.
87