top of page
Home
Trials
Insights
Resources
Best Practices
Tools
Illustrations
Calculators
Webinars
English
عربي
Courses
Groups
Use tab to navigate through the menu items.
ICU LIBERATION
< Back
Play Video
Play Video
05:27
Pain Assessment in the ICU
Accurate pain assessment is paramount in critically ill patients. A range of validated tools can be used in different clinical situations. For those able to express themselves, the Numeric Rating Scale (NRS) and the Visual Analogue Scale (VAS) are commonly used. For patients unable to communicate, tools like the Critical-Care Pain Observation Tool (CPOT) and the Behavioral Pain Scale (BPS) have been designed. Additionally, physiological signs, including changes in heart rate, blood pressure, and pupil dilation, can offer clues, though they often lack specificity and can be influenced by myriad factors
Play Video
Play Video
04:08
Non-pharmacological Interventions in the Management of Pain in the ICU
Non-pharmacological therapy includes massage therapy, cold therapy, music and sound, and relaxation therapy. These interventions can be carried out by nurses and aim to complement pharmacological therapy. Non-pharmacological therapy given to critically ill patients can increase tolerance to pain experienced by disease and procedural pain, reduce physical stress, reduce physical weakness, and minimize the use of analgesic drugs.
Play Video
Play Video
07:15
Pharmacologic Management of Pain in the ICU
The basic principles of pain management in the ICU involve employing an assessment-driven and protocol-based approach. This approach should be holistic, utilizing standardized assessment tools and a combination of non-pharmacological and pharmacological interventions. To enhance the quality of analgesia and reduce side effects, a stepwise multimodal approach to pain management should be implemented. Furthermore, it's important to prioritize analgesia before sedation to minimize the use of sedatives. Special attention should be given to tailoring an individually adapted analgesic regimen, titrating the dosage to specific personalized goals using the lowest effective amount.
Play Video
Play Video
04:27
Richmond Agitation-Sedation Scale (RASS)
The RASS score system, or Richmond Agitation-Sedation Scale is a validated, evidence-based tool employed in the assessment of sedation and agitation in critically ill patients. By providing a standardized measure, it assists intensivists in optimizing patient care, guiding therapeutic interventions, and monitoring patient responses over time
Play Video
Play Video
06:43
ICU Delirium Definition, Etiology, and Outcomes
Delirium is a form of acute brain dysfunction that manifests as fluctuating attention and impaired cognitive function. It can present with a variety of symptoms, including significant psychomotor agitation, depressed level of consciousness, or both. According to the American Psychiatric Association’s Diagnostic and Statistical Manual—5th edition (DSM-5) guidelines, delirium is an acute confusional state defined by acute disturbances in attention, awareness, or cognition developing over hours to days due to disease or sedation that is not better explained by an alternative diagnosis or a comatose state. Notably, delirium can and often does coexist with underlying neurological disease such as dementia, traumatic brain injury, and stroke and so is not precluded from developing in these patients.
Play Video
Play Video
05:48
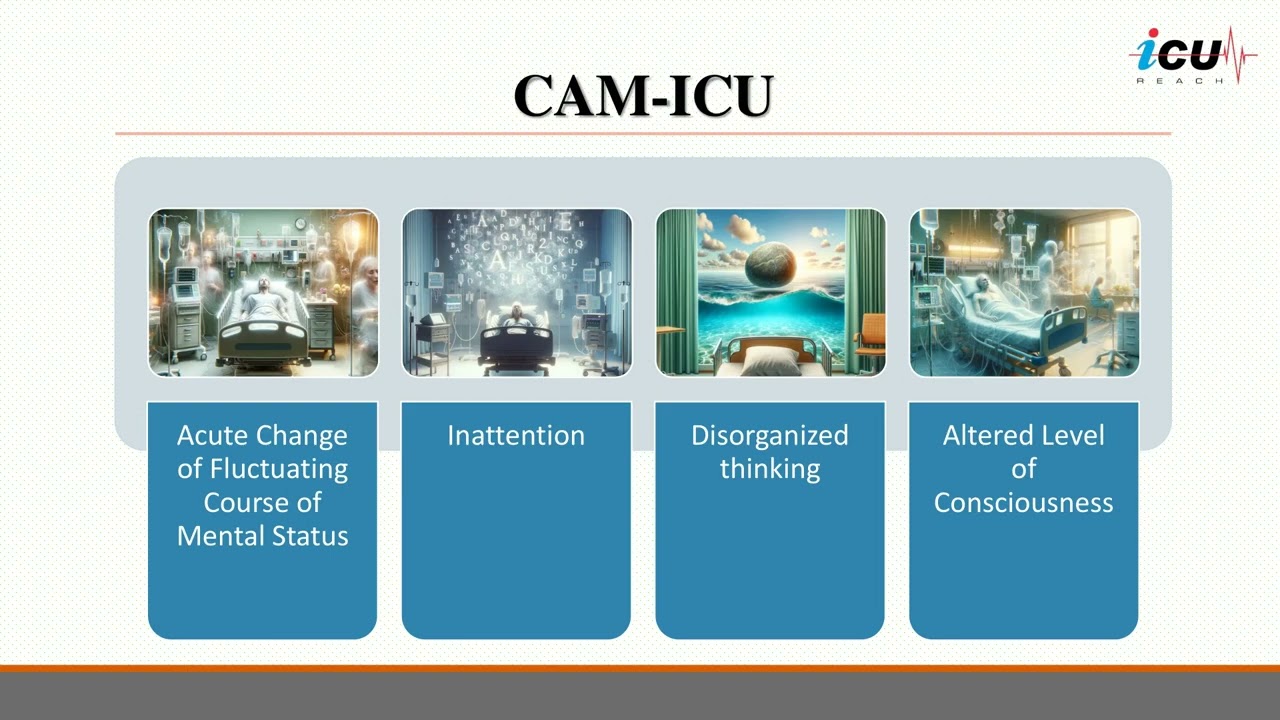
Delirium Screening: CAM-ICU
The Confusion Assessment Method-ICU (CAM-ICU) is extensively validated and used for delirium diagnosis and evaluation of delirium over time. It allows the assessment of attention, orientation, and memory. Of note, this tool allows nonpsychiatric ICU personnel to diagnose the complication rapidly and reliably and can be adopted even when the patient is unable to speak due to endotracheal intubation. The CAM-ICU provides two steps. In the first one, the level of consciousness/arousal is evaluated through a standardized sedation scale such as the Richmond Agitation-Sedation Scale (RASS). This latter is a 10-point scale ranging from +4 to -5, where a RASS value of 0 indicates a calm and alert patient; RASS scores of -4 and -5 are indicative of coma and cannot be further assessed for delirium. All other individuals (moderately sedated, RASS score -3 or more alert) should also be evaluated through the second step assesses patients for four characteristics of delirium. The categories include acute onset of altered mental status, inattention, disorganized thinking, or altered level of consciousness. Three out of four features are required for a diagnosis of delirium. The tools, validated in 1990, has been updated by Marcantonio et al. in 2014, in the 3-Minute Diagnostic Assessment for Delirium (3D-CAM). It is an algorithm easy to perform and can be used by personnel with minimal additional training.
Load More
Support Us
Mail
Log In
bottom of page