
NEJM
January 21, 2023
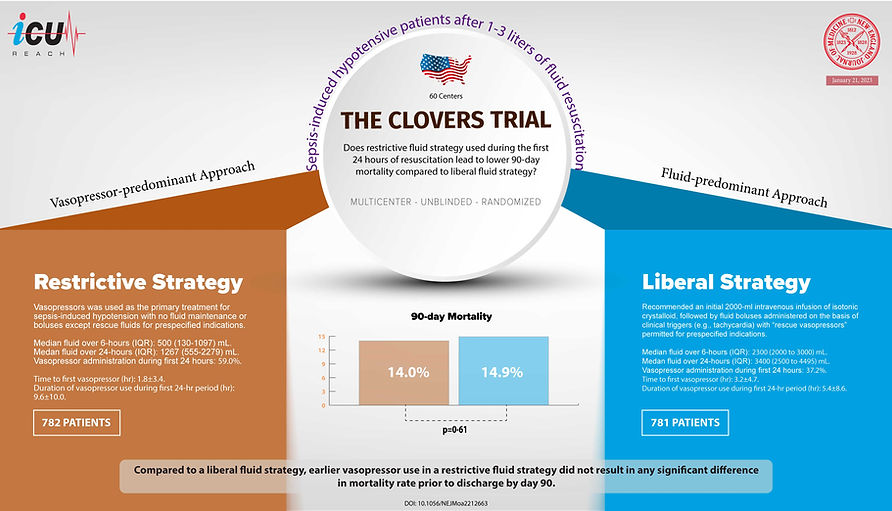
Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension
Mazen Kherallah
Summarized by:
What was the research question?
Does restrictive fluid strategy used during the first 24 hours of resuscitation for sepsis-induced hypotension lead to lower 90-day mortality compared to liberal fluid strategy?
How did they do it?
A multicenter, randomized, unblinded superiority trial at 60 U.S. centers
A total of 1563 patients with sepsis-induced hypotension were randomized after their initial presentation to receive a restrictive fluid strategy (no fluid maintenance or boluses except rescue fluid for prespecified indications with early use of vasopressor, vasopressor-predominant approach, 782 patients) or a liberal fluid strategy (using intravenous fluids before vasopressor use, fluid-predominant approach, 781 patients) for a 24-hour period. Patients in both groups received 1-3 liters of initial resuscitative fluid.
Primary outcome was 90-day mortality, and secondary outcomes included 28-day measures of the number of days free from ventilator use, days free from renal-replacement therapy, days free from vasopressor use, days out of the ICU, and days out of the hospital.
What did they find?
After a thorough evaluation, the data and safety monitoring board recommended that the trial be suspended due to its ineffectiveness in producing different results for primary and secondary outcomes during their second interim analysis.
During the 24-hour time frame, different resuscitation therapies were provided to both groups; with fewer intravenous fluids given in the restrictive fluid group relative to the liberal fluid group (difference of medians, −2134 ml; 95% CI, −2318 to −1949). Additionally, patients within the restrictive fluid cohort experienced earlier application and extended duration of vasopressor use.
There was no statistical difference in the 90-day mortality between the two groups with a mortality rate of 14.0% in the restrictive fluid group compared to 14.9% in the liberal fluid group (estimated difference, −0.9 percentage points; 95% CI, −4.4 to 2.6; P=0.61).
There was no significant difference in the secondary outcomes.
Treatment effects were not different in the prespecified subgroup analyses that included patients with systolic blood pressure of less than 90 mm Hg or receipt of vasopressors at randomization, chronic heart failure, end-stage renal disease, and pneumonia as the cause of sepsis.
With 500 patients received vasopressors through a peripheral catheter, only three instances of extravasation that were able to resolve without any intervention or consequence. This data strongly supports the use of this practice as being safe and reliable.
What are the limitations?
The study was terminated early putting it at risk for type 2 error but it is very unlikely.
Some variations to protocol existed in both groups.
Potential bias due to unblinding nature of the trial.
The two groups were protocolized (guidance was given to the clinicians in two different protocols).
Duration of the protocol was limited to 24 hours only with specific targets. The study does not rule out a different effect should the duration was longer or different targets were used.
This study included patients with initial presentation of sepsis-induced hypotension and ots results cannot be extended to those patient developing sepsis during hospitalization.
What does it mean?
This trial was conducted on patients with septic shock who were resistant to the initial treatment of 1-3L IV fluids. They found that compared to a liberal fluid strategy, using earlier vasopressor use in a restrictive fluid strategy did not result in any significant difference in mortality rate prior to discharge by day 90.
Using restrictive fluid strategy with early vasopressors is safe and has similar outcome to liberal strategy.