
Hypothermia vs Normothermia in Patients With Cardiac Arrest and Nonshockable Rhythm
- Mazen Kherallah

- Dec 28, 2023
- 5 min read
Updated: Dec 30, 2023
Medical guidelines advocate for active prevention of fever in unconscious patients who have been resuscitated following cardiac arrest for a duration of at least 72 hours post-resuscitation. This recommendation underscores the potential negative impact of fever on neurological outcomes and overall recovery in such patients. However, these guidelines also acknowledge a significant gap in the current medical knowledge base: there is a lack of conclusive evidence regarding the benefits or drawbacks of hypothermia through targeted temperature management (TTM) in patients with nonshockable rhythm (NSR) [1].
Compared to patients with shockable rhythms, those patients with cardiac arrest and initial nonshockable rhythm generally have worse neurological outcome and higher mortality rates [2].
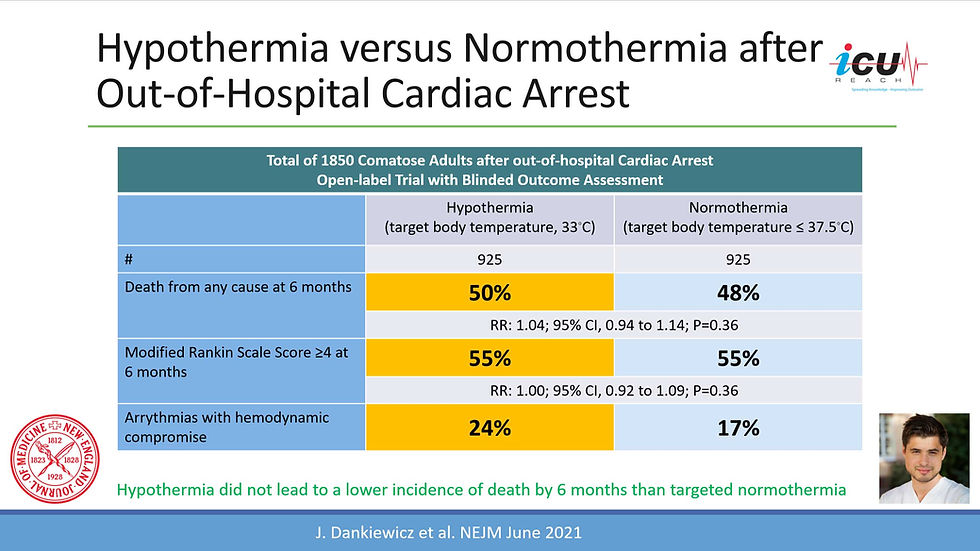
The TTM2 trial, when compared to two other landmark trials [3,4] evaluating the hypothermia in comatose patients after cardiac arrest, distinguished itself with a considerably larger study cohort and more robust methodological approaches, enhancing the reliability and credibility of its findings. There was no benefit on mortality or functional outcomes for hypothermia at 33 °C compared to targeted normothermia at ≤37.8°C in patients with out-of-hospital cardiac arrest. However, only 26% of the trial population had an initial nonshockable rhythms which limits the generalizability of the trial's findings to those patients [5].
The HYPERION trial in 2019 revealed that among patients with coma who had been resuscitated from cardiac arrest with NSR, moderate therapeutic hypothermia at 33°C for 24 hours led to a higher percentage of patients who survived with a favorable neurologic outcome at day 90 than was observed with targeted normothermia [6].

A recent individual patient data meta-analysis integrated findings from the TTM2 and HYPERION, to evaluate the efficacy of hypothermia at 33 °C against controlled normothermia in unconscious adults resuscitated from out-of-hospital cardiac arrest (OHCA) with an initial NSR. The primary objective was to determine if a lower body temperature target could improve survival and functional outcomes. The study included a total of 912 patients, with 490 from the TTM2 trial and 422 from the HYPERION trial [7].
The study analyzed that data in two groups: one receiving hypothermia treatment with a target temperature of 33 °C and the other managed with normothermia, maintaining a body temperature between 36.5 to 37.7 °C, for a minimum of 24 hours. The primary outcome measured was mortality at 3 months post-resuscitation, and the secondary outcome focused on the assessment of unfavorable functional outcomes within 3 to 6 months, characterized by a Cerebral Performance Category score of 3 to 5.
The results showed that 80.1% of patients in the hypothermia group and 82.1% in the normothermia group died within 3 months, indicating no significant difference in survival rates between the two groups (Relative Risk [RR] with hypothermia, 1.04). Similarly, unfavorable functional outcomes were observed in 90.0% of the hypothermia group and 89.2% of the normothermia group, again showing no significant difference (RR with hypothermia, 0.99). These findings led to the conclusion that in unconscious survivors of OHCA with an initial nonshockable rhythm, lowering the body temperature to 33 °C does not significantly enhance survival or functional outcomes when compared with controlled normothermia.
This meta-analysis, the largest of its kind, analyzed data from two major randomized clinical trials to understand the effects of Targeted Temperature Management (TTM) in patients with NSR after cardiac arrest. NSR is particularly important as it is the most common rhythm following cardiac arrest worldwide. While the HYPERION trial indicated some benefits of therapeutic hypothermia in NSR, this meta-analysis suggests otherwise. It underscores that future trials like the ICECAP trial, which aims to explore the benefits of longer-duration therapeutic hypothermia in NSR, might not yield positive results as this meta-analysis indicates no significant benefits in mortality or functional outcome.
The meta-analysis also didn’t find differences in outcomes based on time to return of spontaneous circulation (ROSC), presence of shock, CAHP score, or lactate levels among the 912 patients analyzed. The ICECAP trial, which lacks a normothermia control group, is designed to assess different TTM durations in both shockable and nonshockable rhythms. However, based on this meta-analysis, the effectiveness of cooling to improve outcomes is not convincingly proven and requires further investigation in prospective randomized trials.
Additionally, the meta-analysis did not directly investigate outcomes related to sedation, paralysis, or mechanical ventilation as these measures were not standardized. No differences were observed in the frequency of pneumonia, arrhythmias, or bleeding events. However, the TTM2 trial indicated an increased risk of arrhythmia and other complications like prolonged mechanical ventilation in the hypothermia group, highlighting potential risks of this intervention.
Neuroprognostication accuracy in cardiac arrest outcomes is crucial. Most deaths post-cardiac arrest are due to withdrawal of life-sustaining treatment (WLST) based on perceived poor neurologic recovery prospects. The HYPERION and TTM2 trials differed in their approach to neuroprognostication, which could bias outcome data. This variability emphasizes the need for a standardized and multimodal system in line with current guidelines to avoid bias.
Future studies are advised to focus on fever prevention's role in neurological outcomes post-cardiac arrest. The STEPCARE and upcoming TTM3 studies will explore fever management and the impact of sedation in this context. Long-term follow-up data from the TTM2 trial might also provide valuable insights into patient outcomes, highlighting the need for continued research in this field.
In conclusion, the recent meta-analysis that combined the TTM2 and HYPERION trials suggests limited benefits of lowering targeted temperature management (TTM) to 33 degrees Celsius for cardiac arrest patients in patients with nonshockable rhythms. It seems very reasonable to target a normothermia with a controlled temperature of 36.5 to 37.7 in these patients.
Temperature target for patients with coma after cardiac arrest of nonshockable rhythm should be:
0%36.5 to 37.7 °C
0%34-36 °C
0%32-34 °C
REFRENCES
Sandroni C, Nolan JP, Andersen LW, et al. ERC-ESICM guidelines on temperature control after cardiac arrest in adults. Intensive Care Med. 2022;48(3):261-269. doi:10.1007/s00134-022-06620-5 PubMed Google Scholar Crossref
Grunau B, Reynolds JC, Scheuermeyer FX, et al. Comparing the prognosis of those with initial shockable and non-shockable rhythms with increasing durations of CPR: Informing minimum durations of resuscitation. Resuscitation. 2016;101:50-56. doi:10.1016/j.resuscitation.2016.01.021 PubMed Google Scholar Crossref
.Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549-556. doi:10.1056/NEJMoa012689 PubMed Google Scholar Crossref
Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346(8):557-563. doi:10.1056/NEJMoa003289 PubMed Google Scholar Crossref
Dankiewicz J, Cronberg T, Lilja G, et al; TTM2 Trial Investigators. Hypothermia versus normothermia after out-of-hospital cardiac arrest. N Engl J Med. 2021;384(24):2283-2294. doi:10.1056/NEJMoa2100591 PubMed Google ScholarCrossref
Lascarrou JB, Merdji H, Le Gouge A, et al; CRICS-TRIGGERSEP Group. Targeted temperature management for cardiac arrest with nonshockable rhythm. N Engl J Med. 2019;381(24):2327-2337. doi:10.1056/NEJMoa1906661 PubMed Google ScholarCrossref
Taccone FS, Dankiewicz J, Cariou A, et al. Hypothermia vs Normothermia in Patients With Cardiac Arrest and Nonshockable Rhythm: A Meta-Analysis . JAMA Neurol. Published online December 18, 2023. doi:10.1001/jamaneurol.2023.4820. Link

Comments